
In my last post I wrote way too many words about the measles portion of the MMR vaccine. 🙂 Measles tends to be the attention-getter of this one, (Disneyland anyone?) But the MMR also contains live-virus mumps and rubella and a whole bunch of other interesting and controversial ingredients.
In today’s post about I’m going to talk all things mumps, rubella, rubella in pregnancy, outbreaks, at-home care, and even how my sister found out that she lost all her vaccine-induced rubella immunity when she was tested in pregnancy, 25 years after her MMR vaccine! Of course when she needed it most.
Glad you are here! 🙂
This is Part 8 in my vaccine series discussing which vaccines we decided to give to our children and why. You may also want to check out the other posts in this series:
Part 1: Our Vaccine Choice: Risks, Benefits, Responsibility
Part 2: Hepatitis B and Hib Vaccines
Part 3: Diphtheria, Tetanus and Pertussis Vaccine
Mumps:
Overview: (CDC)
Mumps is a contagious disease caused by a virus. It is spread by saliva, often by sharing utensils, cups, kissing, etc, but can also be spread through sneezing and coughing. When it is experienced in childhood, before puberty it is a harmless disease. Most complications occur in post-pubescent older children and adults. Mumps virus has a very long incubation period and symptoms usually occur 16-18 days after exposure. Full recovery usually occurs in 3-7 days and immunity is lifelong and permanent.
Symptoms:
- Fever and chills
- Headache
- Muscle aches
- Loss of appetite
- Fatigue
- Swollen salivary glands along the jaw line
- In some instances, reproductive glands such as the ovaries and testes may swell.
Symptoms of mumps usually start with gland swelling on the jaw line followed by slight fever. Swelling will go down after 4-5 days. About 1/3 of cases may not have any swelling. Complications from mumps are usually in adults who did not get mumps in childhood or whose vaccine immunity has worn off. These include orchitis or inflammation of the testes (20% of post-puberty male cases,) usually in only ONE testicle. Sterility from mumps is extremely rare. In rare cases, mumps has been associated with temporary hearing loss and aseptic meningitis, a less serious form of meningitis that resolves in 3-7 days. Mumps is very rarely a deadly disease.
Management and At Home Care for Mumps:
- There is no conventional treatment for mumps. It usually just will run its course.
- Basic home care with plenty of fluids, antiviral herbs such as elderberry, and astragalus and echinacea glycerite is helpful. There is a supplement called ACF that we use for practically anything that contains many of these immune boosting properties.
- There is some evidence that high-dose Vitamin C (using lypo-spheric or sodium ascorbate vitamin C) by dosing to bowel tolerance, is very effective in reducing mumps severity and duration.
- Give cod liver oil for Vitamin A and D + anti-inflammatory properties.
- Essential oils (for pain and discomfort in the jaw area: lavender and bay laurel. Dilute 1 drop each in 1/2 tsp of carrier oil.
- For homeopathic therapy, try Parotidinum 30C as a prophylactic protocol to reduce risk and severity of symptoms. Also suggested: Aconitum napellus (Acon) 30C at onset, Arsenicum album (Ars) if discomfort is accompanied by burning pains, or Belladonna 30C if the child’s fever is above 103. For more information about using homeopathy for mumps read: The Unvaccinated Child: A Treatment Guide for Parents and Caregivers.
My Thoughts:
Mumps is mostly seen today in college campuses, camps, and schools in vaccinated populations. It is well known that the mumps portion of the MMR is greatly reduced in its efficacy within 5-15 years. By fifteen years post-vaccine, many kids are in college which is why we see most outbreaks in this population. Like measles and rubella (which you’ll see below) this has shifted the vulnerability to an age group where the disease is more dangerous and complications are likely, although it is observed that previously vaccinated adults may have lesser symptoms.
Because most mumps complications result in boys past puberty, I did not see the urgency in getting my three girls vaccinated against mumps. It is a mild childhood disease and being knowledgeable about the symptoms and treatment options, I felt prepared.
If I had boys, I would be concerned about mumps as he aged past puberty, but again- even in the highly vaccinated population, mumps is a more common issue due to vaccine waning in teenagers and college students. After TWO doses of MMR, test studies showed a range of 31% to 95% effectiveness against mumps. Even with a THIRD dose of MMR as an adult, the ACIP states that effectiveness is 61-88%.
If we had a son, we would reassess at puberty and consider a mumps titer test to see if he developed mumps immunity from childhood exposure before considering vaccination. Unfortunately, since 2009 the ACIP no longer recommends giving single vaccines for mumps, rubella, and measles, so the MMR is the only vaccine available for mumps today.
Rubella:
Overview: (CDC)
Rubella (also called “German Measles”) is a contagious disease caused by a virus. It is spread through respiratory particles from sneezing, coughing, etc. Infections usually occur between late winter and early spring. When it is experienced in childhood, it is mild and goes away on its own in a few days. Up to 50% of rubella cases are so mild that they may go completely unnoticed. Medical intervention is rarely required. The entire illness lasts 5-7 days. Immunity is lifelong in the vast majority of people.
The only population of people that rubella affects harmfully are unborn babies. In 20-25% of cases where women were exposed to rubella for the first time in their first trimester of pregnancy, their baby developed Congenital Rubella Syndrome. (more below)
Symptoms:
- Low to mid-grade fever
- Rash (much fainter and milder than classic measles)
- Sore throat
- Runny nose
- Possible swollen and tender lymph nodes
- Possible tender joints
- In adults only- arthritic feelings in joints and conjunctivitis that resolves within a month in most cases.
Congenital Rubella Syndrome:
In the 1940’s it was first noticed that women exposed to rubella in their first trimester were giving birth to babies with congenital defects such as eye problems and blindness, hearing loss, mental challenges, and heart disease. Defects are rare if the initial rubella infection occurs after 20 weeks of pregnancy. A large outbreak in the mid-1960’s led to the licensing of a rubella vaccine in 1969.
Symptoms of CRS (in infant):
- deafness (the most common complication)
- preterm delivery
- heart defects
- microcephaly
- blindness and eye defects
- bone abnormalities
CRS is the primary reason all children are vaccinated against rubella so early. It is strictly to protect the unborn fetus of pregnant women exposed to rubella. Before a large rubella outbreak in 1964-65, when there were an estimated 12 million cases of rubella and 20,000 babies born with CRS, there was not much talk of CRS. This estimate was taken from one study done in 1966.
I want to note that I searched to no avail for the source of these monstrous numbers in places other than the 1966 study, as they did not line up with the CDC’s actual statistics of typical years of rubella (~50,000 cases per year and ~60 CRS cases- see page 2.) For the years, 1964-65 their statistics are recorded as “NR= not nationally recordable) and it was truly an anomaly if their estimated statistics were indeed 12.5 million cases and 20,000 cases of CRS.
This 1967 paper states that CRS cases were an estimated 10,000-20,000 between 1964-1966. I did note here in this paper that New York City’s CRS statistics were at 1,000 cases, so perhaps they took this statistic and estimated for the rest of the country from there?
Management and At Home Care for Rubella:
- There is no conventional treatment for rubella, although immune globulin may be given to pregnant women suspected of rubella exposure that have a negative rubella antibody titer.
- Basic home care and antivirals such as elderberry, and astragalus, echinacea and osha glycerites would be helpful. My favorite supplement for acute immune support- ACF has all of these.
- Essential oils such as German chamomile, tea tree, and lavender will help with any itch and are antiviral. Use two drops of each oil in 2 tsp of carrier oil and wear gloves to apply to child.
- I would also consider an over the counter anti-itch cream if the child is extremely uncomfortable. Rest is essential to recovery.
- The homeopathic prophylaxis used for rubella is Rubeola (Rubeol) 30C. This will reduce severity of symptoms and duration. For rubella with rapid onset of symptoms try Acon 30C and Belladonna 30C. For more information about using homeopathy for rubella read: The Unvaccinated Child: A Treatment Guide for Parents and Caregivers.
My Thoughts:
As many of you know, we have three daughters so rubella and CRS were things I was concerned about when I first began my vaccine research. Also, as a woman of childbearing age I was concerned for my unborn children. A simple rubella titer test given during prenatal care as standard of care in the U.S. will give you an idea of how strong your rubella immunity is.
Some women may choose to test for this BEFORE becoming pregnant. I actually strongly advise this, as the rubella vaccine in some vaccinated women wear off by the time you reach childbearing age. This happened to my sister who found during her prenatal care with her first child that her rubella immunity from her childhood-MMR had waned and she was no longer immune.
Even though rubella has been eradicated since 2004 in the U.S., there are still cases of rubella circulating. Due to the mild nature of the disease, these often go unreported. We also need to be reassured that until 1964-65, CRS cases were a rarity and not even reported nationally. Most of these cases (40-50%) resulted in hearing disabilities, but other more severe difficulties were reported as well.
Unfortunately, since 2009 the ACIP no longer recommends giving single vaccines for mumps, rubella, and measles, so the MMR is the only vaccine available for rubella today.
Our Decision:
If you already read my last post where I talk about our decision regarding the MMR vaccine, then you you know we decided to forgo the MMR vaccine for our children altogether. Out of these three illnesses, we were most concerned about rubella as our three daughters reach adulthood.
Our plan is to forgo any vaccination for rubella and see if they contract it as children for natural immunity (since rubella is extremely mild in childhood and before the vaccine, 85% of children conferred natural immunity). We will get their antibody levels tested as pre-teenagers to see if they have rubella immunity and then go from there, considering educating them about the MMR as an option before pregnancy as they get older if they do not show rubella immunity.
Unfortunately, if they were to receive the MMR as an adult, they are much more likely to develop symptoms of acute arthritis after receiving the rubella portion of this vaccine which is also a symptom of rubella itself. 25% of adult women who receive the rubella vaccine experience this side effect, some of which results in ongoing, chronic arthritis.
This vaccine is a tough one to decide about. In my post about measles and MMR, I went over in more detail our convictions about this vaccine in relation to cancer and other issues that are becoming more prevalent in children today.
What I have said today regarding rubella non-vaccination in my young daughters may come off as insensitive to pregnant women, but it should be known that when the rubella vaccine was introduced in 1969, the U.S. and U.K. differed on their vaccination strategy. The U.K chose to vaccinate teenage girls:
In the United States, the strategy was to vaccinate infants, so that eventually the reservoir in childhood would be abolished [52]. In contrast, the United Kingdom decided on a program of vaccinating adolescent girls [53]. Both strategies were partial successes, in that CRS incidence began to decrease. However, both were also partial failures, because in the United States pregnant women were still being exposed to rubella in children and adults, and in the United Kingdom unvaccinated girls who refused vaccination were still exposed to rubella cases….”
–Clinical Infection Diseases, Dr. Stanley Plotkin
I firmly believe that (even as a currently pregnant woman as I write,) it is the responsibility of a young woman who may become pregnant, regardless of vaccination status, to be proactive in assessing her risk of rubella infection during pregnancy. Immunity can be assessed through prenatal testing of rubella antibodies during standard prenatal care.
Even if you find that your immunity to rubella is low, if you look at pre-vaccine numbers and estimates, the chances of having a baby born with CRS were incredibly low. 1969 numbers reported 62 cases of CRS (you can look at the entire record of cases on the right side of this document) and before the “anomaly” years of 1964-65, cases were not even recorded.
Overall, rubella is extremely puzzling. What exactly happened in 1964-65 to cause such a rise in cases that hadn’t ever happened before? No one seems to have a great answer, but it is comforting to know that today we have options to protect ourselves and our children.
MMR and MMRV Vaccines:
The Mumps and Rubella vaccines were introduced in 1967 and 1969. Today they are no longer offered in their single dose format so doctors and clinics will offer the MMR and MMRV below.
Ingredients:
- Measles and mumps viruses taken from individuals in the 1960’s. The rubella virus was taken from an aborted human fetus (scientifically named WI-38) in the 60’s. You can read the story of the Swedish married mother who aborted her female baby at 4 months gestation HERE.)
- culture of human lung cells (from WI-38 above)
- traces of chicken embryo cells
- Inactive Ingredients: sorbitol, sodium phosphate, potassium phosphate, sucrose, sodium chloride, hydrolyzed gelatin, recombinant human albumin, fetal bovine serum, other buffer and media ingredients, neomycin (antibiotic)
- The same measles, mumps, and rubella viruses from the MMR II above with added varicella (chickenpox) virus
- sucrose
- hydrolyzed gelatin
- urea
- sodium chloride
- sorbitol
- monosodium glutamate (0.4 mg)
- sodium phosphate dibasic
- recombinant human albumin (residual DNA from the lung of a 14 week male human fetus scientifically named MRC-5 aborted from a 27 year old psychiatric patient in 1966.)
- sodium bicarbonate
- potassium phosphate
- potassium chloride
- potassium phosphate dibasic
- bovine serum
- neomycin
Aborted Fetal Tissue in Rubella, Varicella, and Hepatitis A Vaccines:
The MMR II has been in use since the early 1990’s. The original MMR was released in 1963 and became commonly used by the late 60’s. It is one of the vaccines (the others being Hep A, shingles, chickenpox, rabies, and adenovirus,) that contain human aborted fetal cells in its production (WI-38 female fetal lung tissue cell line).
The MMRV contains MMR + Varicella (chickenpox) which contains a different strain of aborted fetal tissue in addition to the WI-38 in the MMR. Therefore the MMRV (ProQuad) contains TWO strains of aborted fetal cells and its DNA (WI-38 female cells and MRC-5 male fetus cells.)
Both vaccines contain the WI-38 female strain of lung-diploid tissue. To get to the point where they were finally successful with culturing the rubella virus in WI-38 to make the vaccine, it took dozens of abortions in trial and error. After being exposed to rubella in the 1st trimester, 26 mothers were told their babies were likely to have congenital rubella syndrome (CRS) and would be born with deformities and would likely die. With this “knowledge”, they elected to have an abortion, but it wasn’t until the 27th baby was aborted that a baby with CRS was discovered. That baby, originally named RA273 (R=Rubella, A=Abortus, 27=27th fetus, 3=3rd tissue explant) was renamed WI-38, was dissected, and cell lines from its lung tissue is what we inject in children today in the MMR and MMRV vaccines. (Source – from original 1960’s paper.)
How long does immunity last with the two series MMR?
It does not confer permanent immunity in all individuals and large, long-term studies testing immunity have not been conducted, although the CDC states that it is 97% effective for measles and rubella and 88% effective for mumps (these were averaged from a range of responses in test individuals.)
I have read one article suggesting immunity lasts 20 years but cannot find any studies testing antibody response in the long term (over 20 years). Why is it so hard to find these studies? If you come across any, please feel free to message me. 🙂
Adverse Reactions Reported after MMR and MMRV:
The possible complications with the MMR or MMRV are similar to the actual infections of the viruses they are designed to protect against.
Some of the top reactions listed are (from the CDC website):
- Sore arm from the injection
- Fever
- Redness or rash at the injection site
- Swelling of glands in the cheeks or neck
- Seizure (jerking or staring) often associated with fever
- Temporary pain and stiffness in the joints, mostly in teenage or adult women
- Temporary low platelet count, which can cause unusual bleeding or bruising
- Rash all over body
- Deafness
- Long-term seizures, coma, or lowered consciousness
- Brain damage
MMR and MMRV Safety:
It is important to know that very few vaccines (none that I could find that are given in the U.S.) have been exclusively tested against a saline placebo for testing.
Below is just one of the several studies for safety the MMRV (ProQuad) underwent. They compared children just given the ProQuad with children given the two separate vaccines of MMR II + Varicella. You can read more about the safety studies conducted in the actual vaccine inserts above.
“ProQuad was administered to 4497 children 12 through 23 months of age involved in 4 randomized clinical trials without concomitant administration with other vaccines. The safety of ProQuad was compared with the safety of M-M-R II and VARIVAX given concomitantly (N=2038) at separate injection sites. The safety profile for ProQuad was similar to the component vaccines. Children in these studies were monitored for up to 42 days post-vaccination using vaccination report card-aided surveillance. Safety follow-up was obtained for 98% of children in each group.”
It is also important to note that many of these studies (if not all) did not follow up with LONG TERM problems of vaccinated children.
Clinical trials for vaccine approval are almost always done comparing the vaccine that is up for approval with ANOTHER similar vaccine- with all participants often given other additional vaccines as well. They do not use a saline placebo like other drug trials, as it is considered “unethical” and “a threat to public and individual health” to withhold a vaccine from a test subject.
There were a few vaccine studies I was able to find that were conducted in the manner of double-blind, placebo-controlled, but they were mostly for vaccines and researchers not from the U.S. I imagine there were a few more, but you can see a concise list of those HERE. None of them were the MMR or MMRV.
Concerns about Childhood Cancer
From the MMR and MMRV vaccine inserts:
“M-M-R II has not been evaluated for carcinogenic or mutagenic potential, or potential to impair fertility.”
“ProQuad has not been evaluated for its carcinogenic, mutagenic, or teratogenic potential, or its potential to impair fertility.”
With childhood cancer up 27% since 1975, wouldn’t it be wise to look into the relation between cancer and vaccines with a little more enthusiasm?
Childhood cancer is unique in that it is strictly thought to be the result of DNA changes early in childhood and not due to lifestyle and environmental changes like adult cancers. One would think that injecting children with fragments of cow, chicken, monkey, and both male and human fetal DNA to freely act on our own DNA would result in mutagenic occurrence, such as this study observes.
Dr. Theresa Deisher, Ph.D. genetic engineer, by far has the best explanation of the dangers of this related to vaccines and this entire video series is worth the watch.
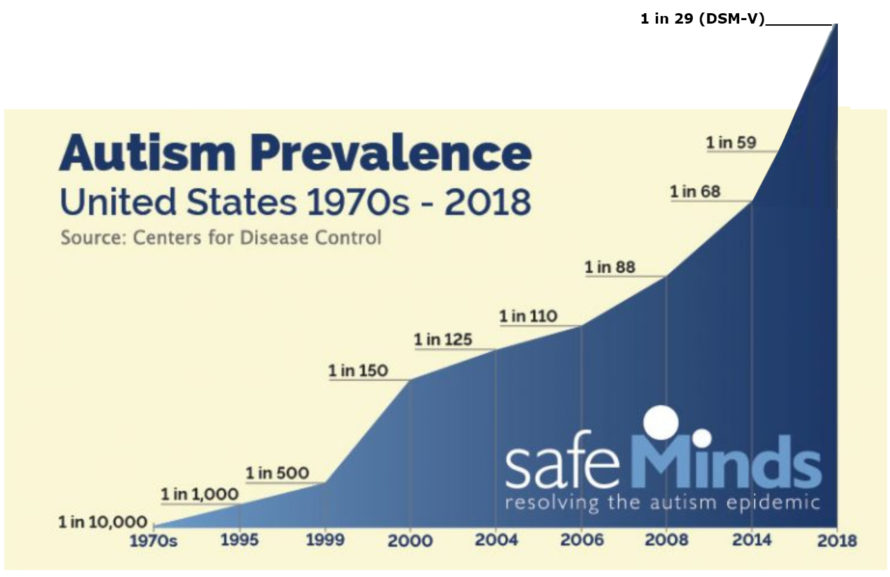
Autism statistics and projections. Some studies place us at 1 in 36 today.
Concerns about Autism
I could go on and on about the MMR and studies both proving and disproving its involvement in the rise of childhood autism. Instead, I’m just going to provide some of these studies (both supportive and some disproving of the theory) and encourage you to read on your own.
The autism community buzzes with this debate, many families claiming with great confidence that their child regressed into their autistic state after their MMR or another vaccine. You can watch dozens of these stories at VAXXED TV.
The fact is, that in the 1940’s, autism was practically unknown and there were a handful of cases (when vaccines were first officially recommended for school- although only the DPT and smallpox vaccine- and not everyone could afford or received it.)
Autism was so rare at that time that Dr. Leo Kanner, the father of American childhood psychiatry, described the disorder as “a behavior pattern not known to me or anyone else theretofore.”
Statistics gradually and then rapidly increased starting in the 1980’s.
Today the 2017 official autism statistics from the CDC are 1 in 59 (with the NCHS finding 1 in 36 in 2016.)
Abnormal MMR antibodies in children with autism
http://www.ncbi.nlm.nih.gov/pubmed/12145534
Tylenol, MMR and Autism – A parent survey study
http://www.ncbi.nlm.nih.gov/pubmed/18445737
Rebuttal of the “Taylor Study” by Autism dad, J.B. Handley
Subtle DNA changes and the overuse of vaccines in autism
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3364648/
Vaccine and Autism- a New Scientific Review (article)
http://www.cbsnews.com/…/vaccines-and-autism-a-new…/
Summary of previous Journal of Immunology
http://danmurphydc.com/…/AR-10-12-rata-AUTISM-VACCINE.pdf
Autism and Resulting Medical Conditions:
http://www.tacanow.org/…/09/autism-studies-april-2008.pdf
Mercury toxic encephalopathy manifesting with clinical symptoms of regressive autistic disorders. http://www.ncbi.nlm.nih.gov/pubmed/17454560
Relation of mercury to high autism rates in boys
http://www.ncbi.nlm.nih.gov/pubmed/16264412
A Positive Association found between Autism Prevalence and Childhood Vaccination
http://www.ingentaconnect.com/…/00000014/art00002…
Peer reviewed study on fetal cell contamination with retro virus associated with autism and cancer
http://www.globalresearch.ca/new-study-in-journal…/5402912
Autism and mercury poisoning
http://www.ncbi.nlm.nih.gov/pubmed/11339848
Hypothesis: conjugate vaccines may predispose children to autism spectrum disorders
http://www.ncbi.nlm.nih.gov/pubmed/21993250
This study provides new epidemiological evidence supporting an association between increasing organic-Hg exposure from Thimerosal-containing childhood vaccines and the subsequent risk of ASD diagnosis. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3878266/
This study suggests that although mercury has been removed from many vaccines, other culprits may link vaccines to autism. Further study into the relationship between vaccines and autism is warranted. http://www.ncbi.nlm.nih.gov/pubmed/21623535
This article discusses the data that Dr. Brian Thompson first told Dr S Hooker, a researcher on autism, about the manipulation of a CDC study he was a member of in 2004. Hooker analyzed the raw data from the CDC study afresh and confirmed that the risk of autism among African American children vaccinated before the age of 2 years was 340% that of those vaccinated later. http://www.ncbi.nlm.nih.gov/pubmed/25377033
This looks at a study conducted directly by CDC epidemiologists but greatly ignored that shows a 7.6-fold increased risk of autism from exposure to Thimerosal during infancy. http://www.ncbi.nlm.nih.gov/pubmed/24995277
Boys vaccinated as neonates had threefold greater odds for autism diagnosis compared to boys never vaccinated or vaccinated after the first month of life. http://www.ncbi.nlm.nih.gov/pubmed/21058170
A study that results showed how children from countries with the highest autism spectrum disorder prevalence appear to have the highest exposure to aluminum from vaccines http://www.ncbi.nlm.nih.gov/pubmed/22099159
Study that found that mercury exposure (and the inability to excrete it after injection) is capable of causing some autism spectrum disorders. http://www.ncbi.nlm.nih.gov/pubmed/19106436
The role of thimeresol (mercury) and lack of exretion and autism specturm disorder: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3774468/
This study compares siblings (one autistic and one not) and proposed that those with a mild mitochondrial defect may be highly susceptible to mitochondrial specific toxins like the vaccine preservative thimerosal: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3697751/
Discussion of documented causes of autism include genetic mutations and/or deletions, viral infections, and encephalitis following vaccination. http://www.ncbi.nlm.nih.gov/pubmed/21299355
A look at conjugate vaccines as a cause of autism: http://www.ncbi.nlm.nih.gov/pubmed/21907498
This study evaluated the relationship between prenatal mercury exposure from thimerosal (49.55% mercury by weight)-containing Rho(D)-immune globulins (TCRs) and autism spectrum disorders: http://www.ncbi.nlm.nih.gov/pubmed/17674242
A look at steroid involvement in the treatment of autism spectrum disorder and thimerosal toxicity: http://www.ncbi.nlm.nih.gov/pubmed/15780490
A look at autism and various causes of neurotoxicity: http://www.ncbi.nlm.nih.gov/pubmed/19043938
The role of mercury in the pathogenesis of autism: http://www.ncbi.nlm.nih.gov/pubmed/12142947
A thimerosal study on mice and neurotoxicity: http://www.ncbi.nlm.nih.gov/pubmed/24675092
*************************************************************
Studies Disproving the Vaccine-Autism Claim:
There are at least 17 studies which are often quoted as proving vaccines do not cause autism. These studies represent the most often cited papers by scientists, public health officials and members of the media when trying to refute any evidence of an association between vaccinations and autism.
I think reading these individually is an important part of a decision regarding vaccines:
14 Studies Disproving the Vaccine-Autism Link + the more recent and widely publicized and quoted “Taylor Study”
http://www.ageofautism.com/2011/07/part-1-.html
http://www.ageofautism.com/2011/07/part-2-.html
http://www.ageofautism.com/2011/07/part-3-.html
http://www.rescuepost.com/…/vaccines-and-autism…
http://www.vaxchoicevt.com/…/Analysis-of-JAMA-Study…
From Age of Autism: “There are serious methodological limitations, design flaws, conflicts of interest or other problems related to each of these 16 studies. These flaws have been pointed out by government officials, other researchers, medical review panels and even the authors of the studies themselves. Taken together, the limitations of these studies make it impossible to conclude that thimerosal and MMR vaccines are not associated with autism.”
VAERS Report:
In 2015, there were ~3,176 adverse events and 11 deaths were reported to the Vaccine Adverse Event Reporting System (VAERS) after completion of MMR vaccine. (Remember this reported number is estimated to be 10-100 times less than the actual number and is a volunteer-based reporting system.)
In 2016, these numbers showed a decrease at ~2,797 adverse events and 6 deaths reported after MMR vaccination.
For the Proquad MMRV there were 2,027 adverse event and 1 death reported in 2015 and 2,173 adverse events and 4 deaths reported in 2016.
Also remember that there are 5-6 other vaccines given at the same time at the 12-month visit, so until there are studies showing INDIVIDUAL vaccine safety studies, we won’t know what truly caused these adverse reactions.

Thank you for all the time you spend researching and writing. We are trying to make informed decisions regarding vaccinations for our child. I would be quick to get on board the anti-vaccine train while my husband believes we should just follow the traditional schedule. The information you provide has limited our debates on this stressful topic. It is so appreciated!
Just felt the need to THANK YOU for all the precious info you share Cortney. God bless you!
You are so welcome!!!! ❤️
Hi Cortney,
I love your website. Thank you for all the hard work that went into researching this information and then writing about it in a way that shows how reasonable and rational is the position of those are skeptical of vaccine safety and vaccine “science.” My daughter had troubling vaccine reactions, and I have had 20 years of chronic fatigue that I believe was triggered by a vaccine (received the rubella vax 2x in 4 years, onset of fatigue followed the 2nd time). I can’t prove it, but there is evidence of a link. Your blog is just what I think I would write if my brain worked properly (ha ha). Keep at it! God bless you and your family.
Beth, I am so sorry to hear about that. Vaccine reactions happen all the time, but since they aren’t acute and most doctor’s nor parents use VAERS frequently, we are at fighting an up hill battle. Thank you for your story. It will relate to others I’m sure. ❤️